
Antenna Evolution: What This Image Shows and Why It Matters
📱↔️📶 The Changing Face of Phone Design
-
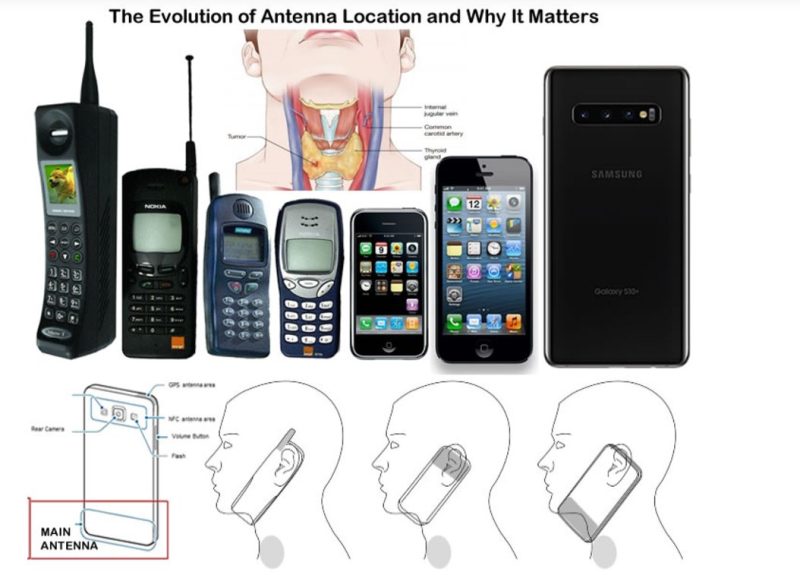
1990s–Early 2000s:
Phones were short, chunky, and the antenna was always at the top—sometimes external, sometimes stubby, but always as far as possible from your neck.-
Why? Because the highest SAR readings (and regulatory focus) were about protecting the brain. The ear/skull phantom was the “danger zone” in early science and litigation.
-
-
2000s–2010s:
As phones slimmed down and screens grew, antennas became internal—but still clustered towards the upper third. -
2015–Now (the 6-inch+ era):
Phones like the Samsung S10+ (and many recent models) moved the main cellular antenna to the bottom bezel—right where the device naturally rests against your neck and thyroid when you hold it to your ear.-
Why? For better reception, space for cameras, and—crucially—to manipulate SAR test results, as we’ll see.
-
🦠 The Anatomy Overlap: Thyroid in the Crosshairs
-
The center overlay shows a classic thyroid cross-section. The thyroid sits just under the skin, unshielded by bone.
-
Modern antenna placement (see lower illustrations) means the main RF “hotspot” is now right against the thyroid—not the skull.
2. The SAR Testing Shell Game
🧪 How SAR Was Meant to Work (and Where It Went Wrong)
-
Original SAR standards (early ’90s):
Phones were tested at the ear, where the antenna was. Head SAR was the safety metric, as the brain was seen as most vulnerable. -
The “phantom” head:
SAR dummies simulate a human skull, filled with liquid to mimic tissue absorption. The focus: energy absorbed by the brain. -
Body SAR:
Later, phones were also tested at the “body” (e.g., in a holster)—but manufacturers could choose a test distance between 5 and 15 mm. This was a relic from the belt-clip era, before pocket or direct-skin use was common.
🎩 The Loophole
-
Move the antenna down:
Now, during head-SAR tests, the ear phantom is farther from the main antenna, so the measured head SAR drops. Great for marketing. -
But reality is different:
When you make a call, the phone’s bottom bezel sits snug against your neck, exactly where the main antenna now is.
Key Point:
Phones haven’t gotten safer. The radiation hotspot has simply migrated—from your skull to your thyroid.
3. The Inverse Square Law and Real-World Exposure
📏 What Distance Really Means for Exposure
-
SAR falls off with the square of the distance:
Doubling the distance between the antenna and your body can quarter the absorbed dose. -
A phone tested at 15mm for body SAR, but used at 0–5mm (in a pocket, on your neck), exposes you to far more RF than the spec sheet suggests.
-
Antenna at the bottom means your unprotected thyroid is now the “closest tissue”—not your thick, bony skull.
4. Why the Thyroid Is So Vulnerable (And What New Science Shows)
🦋 Why the Thyroid?
-
No skull, minimal soft tissue—nothing to block RF energy.
-
Highly vascular and iodine-rich—excellent RF absorber.
-
Critical for childhood development, metabolism, and brain function.
🧬 The New Evidence
-
2025 Ramelet et al. study (rats, 5G at 3.5 GHz, 1.5 V/m):
-
Larger follicles, more colloid, but lower activation index—classic signs of underactive (hypo-) thyroid.
-
Hypothyroidism in children/teens: growth delays, mood disorders, cognitive impairment, and metabolic issues.
-
Structural hypo-activity after only 2 weeks of exposure. Imagine years of real-world use, during development.
-
🔬 Other studies (as referenced above) tie chronic RF exposure to gene expression changes, altered neurotransmitter balance, and even social/behavioral instability.
5. What About “Low-SAR” Phones? The Real Trick
🧮 Marketing vs. Reality
-
Apple tests at 5mm; Samsung often uses 15mm.
-
Lower SAR at 15mm looks “safer” on paper but is meaningless if the phone is in your pocket or pressed to your neck.
-
-
Some companies move the antenna to the bottom, so head SAR drops—even if the thyroid (never measured) is hit with higher doses.
🤔 The Real-World Consequence
-
Consumers, thinking they are choosing a safer phone, may end up increasing their risk by picking a model with a bottom antenna and “low” head SAR.
6. Policy and Practical Takeaways
⚖️ Policy
-
Require SAR mapping for the thyroid and neck—not just the head and “body.”
-
Mandate 0–5mm testing for ALL user scenarios (hand, pocket, call).
-
Close the separation loophole—no more “belt holster” legacy testing in a pocket and neck world.
🛡️ What Can You Do?
-
Use speakerphone or a headset whenever possible.
-
Don’t press the phone’s bottom edge against your neck—especially for long calls.
-
Shielding cases that protect the lower bezel can help (check independent lab tests).
-
Educate kids: phones away from the neck/throat, and never “tucked” for gaming or streaming.
7. The Bigger Story: Design for Safety, Not Just Signal
Every phone is a radio transmitter. Every design choice—antenna placement, testing distance, reported SAR—shapes who absorbs what, and where.
The “low SAR” marketing is a trick of geometry and measurement, not genuine safety. In the age of 5G and ever-larger screens, the radiation bullseye has moved quietly down our faces—directly onto one of our body’s most essential, least protected glands.
In Summary (🔑 Takeaways):
-
Old SAR tests only protected your brain—new phones target your neck.
-
“Low SAR” doesn’t mean “low risk.”
-
The thyroid is especially vulnerable: thin skin, high blood flow, critical for health.
-
Recent animal studies show real biological effects—hypo-thyroid structure after just 2 weeks.
-
Testing and design standards must catch up, or the next generation pays the price.
For more: See Ramelet et al., 2025, Annales d’Endocrinologie, and check rfsafe.com for ongoing advocacy, policy updates, and practical tools for safer wireless living.






