
For years, the public has been told a simplified story about cell phones, cordless phones, Wi-Fi, and radiofrequency radiation: if there were a real cancer problem, brain tumor rates would obviously be rising.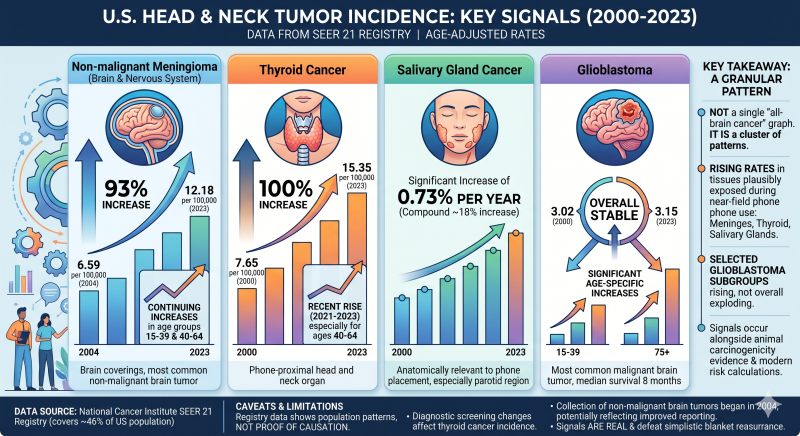
https://www.saferemr.com/2015/05/brain-tumor-rates-are-rising-in-us-role.html
That talking point collapses once the actual tumor categories are examined.
The issue is not just “brain cancer” in the broadest possible sense. The issue is the specific tumors and tissues that matter most in relation to wireless-device exposure: meningioma, glioblastoma, thyroid cancer, salivary-gland cancer, pediatric and young-adult central nervous system tumors, and non-malignant brain tumors that are too often left out of public conversations.
The United States is seeing real population signals in these categories. These signals are visible in age-adjusted cancer-registry data, meaning the increases are not simply explained away by the population getting older. The National Cancer Institute’s SEER November 2025 submission includes SEER 21 data from 2000–2023, with the SEER 21 limited-field database covering approximately 47.9% of the U.S. population and containing more than 18.8 million tumor records.
The numbers demand attention.
The strongest brain-tumor signal: non-malignant meningioma
The clearest and most important brain-tumor signal is non-malignant meningioma.
Meningioma forms in the meninges, the membranes covering the brain and spinal cord. These tumors are often labeled “non-malignant,” but that word can mislead people. A non-malignant brain tumor can still press on the brain, damage nerves, require surgery, recur, and permanently alter a person’s life.
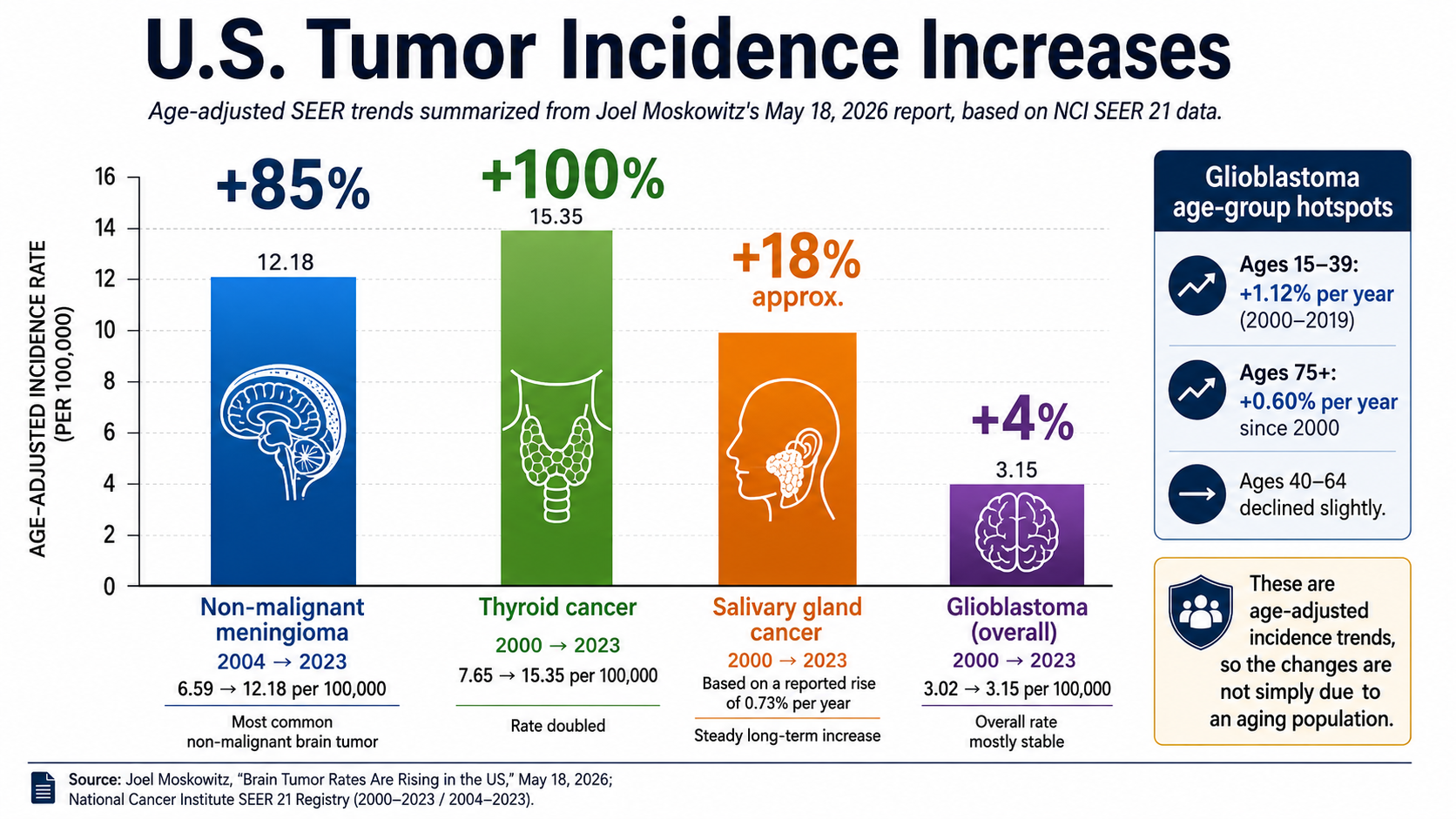
In U.S. SEER data, non-malignant meningioma of the brain and nervous system rose from 6.59 cases per 100,000 people in 2004 to 12.18 cases per 100,000 people in 2023. The increase persisted through 2023 in two major age groups: ages 15–39, rising 1.27% per year since 2009, and ages 40–64, rising 1.97% per year since 2008.
That is not a trivial signal. That is a major population-level increase in the most common brain-tumor category.
The Central Brain Tumor Registry of the United States confirms why this matters. In its 2024 statistical report, CBTRUS reported that from 2017–2021, 72.9% of all primary brain and other central nervous system tumors were non-malignant, making non-malignant tumors more than twice as common as malignant tumors. The same report found that meningioma was the most common predominantly non-malignant histopathology, accounting for 41.4% of all brain/CNS tumors and 56.8% of all non-malignant tumors.
This is the public-health blind spot: when officials or commentators talk only about malignant brain cancer, they leave out most brain and central nervous system tumors. They leave out meningioma. They leave out the category where the increase is most obvious.
Thyroid cancer has doubled since 2000
The thyroid is not deep inside the skull. It sits in the neck — exactly the kind of tissue that should be included when discussing head-and-neck exposure from phones, wireless devices, and chronic radiofrequency radiation.
U.S. SEER data show that thyroid cancer increased from 7.65 cases per 100,000 people in 2000 to 15.35 cases per 100,000 people in 2023 — a doubling over the period examined. The rate rose sharply from 2000–2009, continued rising from 2009–2014, declined from 2014–2021, and then rose again from 2021–2023 at 5.10% per year, with the recent increase concentrated mainly among people ages 40–64.
This is a major head-and-neck tumor trend. Thyroid cancer has been one of the most important cancer-incidence stories of the last generation, and it belongs in any honest discussion of wireless-era health surveillance.
Salivary-gland cancer is also rising
The salivary glands are directly relevant to cell-phone exposure because a phone held against the side of the face places the parotid and salivary-gland region close to the radiation source.
U.S. SEER data show that salivary-gland cancer increased significantly from 2000–2023, with the age-adjusted incidence rate rising 0.73% per year.
That increase is smaller than the meningioma and thyroid signals, but it is important because the location is biologically and anatomically relevant. When people hold phones against the side of the head, the salivary-gland region is one of the tissues most directly exposed.
Glioblastoma: the most aggressive brain cancer is not flat in every age group
Glioblastoma is the most common malignant brain and nervous-system tumor, and it is one of the most devastating cancers a person can receive. The SEER-based data show that the overall U.S. age-adjusted glioblastoma rate was 3.02 per 100,000 in 2000 and 3.15 per 100,000 in 2023. But the age-specific pattern is critical: glioblastoma increased 1.12% per year among young adults ages 15–39 from 2000–2019, and 0.60% per year among adults ages 75 and older since 2000.
This is exactly why broad averages can mislead the public. A total population rate can look relatively stable while important age groups show increases. If exposure, latency, susceptibility, and diagnosis patterns differ by age, then age-specific signals matter.
CBTRUS’s newest report reinforces the severity of the glioblastoma burden: in 2025, an estimated 13,930 new glioblastoma cases are expected in the United States.
Children and young adults are part of the signal
The public also needs to understand what is happening in children, adolescents, and young adults.
A CDC-linked pediatric cancer analysis covering 2001–2014 found that overall pediatric cancer incidence increased by 0.7% per year, central nervous system neoplasms increased by 0.4% per year, and thyroid carcinomas increased by 4.8% per year.
The Annual Report to the Nation also reported that among children ages 0–14, overall cancer incidence increased during 2013–2017, and brain and other nervous-system cancers were among the most common childhood cancers, with increasing trends averaging 0.7%–0.8% per year during 2001–2017.
These are not abstract numbers. They represent children, teenagers, young adults, families, surgeries, radiation treatments, neurological damage, fertility concerns, lifelong monitoring, and deaths.
CBTRUS reported that among children ages 0–14, brain and other CNS cancer was the most common cause of cancer death, and among adolescents and young adults ages 15–39, it was the second most significant contributor to cancer death.
The “non-malignant” category is not harmless
One of the most misleading features of the public conversation is the way non-malignant brain tumors are minimized.
Non-malignant does not mean safe. It does not mean irrelevant. It does not mean “not a real brain tumor.” A tumor growing inside the skull can create serious medical harm even when it is not classified as malignant cancer.
CBTRUS reported that from 2018–2022, non-malignant brain tumors had a statistically significant increase in incidence from 2004–2008 and from 2008–2018, followed by a slight non-significant decrease from 2018–2022.
The 2024 CBTRUS report also found that non-malignant brain and CNS tumors increased significantly from 2004–2009 and again from 2009–2021.
That is the pattern: malignant brain tumors do not tell the whole story. Non-malignant brain tumors are the majority of brain/CNS tumors, and meningioma is the biggest category.
The tumor trends line up with a much larger scientific warning
The population data are alarming on their own. They become even more serious when placed next to the animal evidence and modern risk-assessment evidence.
The U.S. National Toxicology Program completed major radiofrequency-radiation studies in 2018. NIEHS describes those NTP studies as the most comprehensive animal assessment to date of health effects from radiofrequency radiation used in 2G and 3G cell phones. NTP found clear evidence of an association with malignant schwannomas of the heart in male rats, some evidence of malignant gliomas in the brains of male rats, and some evidence of adrenal-gland tumors in male rats. NIEHS also states that the findings challenge the long-held assumption that radiofrequency radiation is not a concern as long as it does not significantly heat tissue.
A WHO-commissioned animal-cancer systematic review published in Environment International reported high certainty of evidence for increased heart schwannomas in male rats and noted that the high-certainty animal tumor types overlap with tumor types where IARC had previously found limited evidence in humans. The same review states that it was partially funded by the WHO radioprotection programme.
Then in 2026, Ronald L. Melnick and Joel M. Moskowitz published a risk-assessment paper in Environmental Health applying benchmark-dose methods to animal cancer data and uncertainty-factor methods to male reproductive toxicity. Their conclusion is stark: current general-public RF exposure limits are 15- to 900-fold higher than their estimates for exposure levels associated with a 1-in-100,000 cancer risk, and 8- to 24-fold higher than levels protective of male reproductive health.
The same paper reports that the health-protective whole-body exposure values they derived — about 0.8 to 5 mW/kg for cancer risk and 3.3 to 10 mW/kg for male fertility — are far below the current FCC/ICNIRP general-public whole-body limit of 0.08 W/kg, or 80 mW/kg.
That is the core public-health problem: current exposure limits were built around short-term heating assumptions, not modern cancer-risk assessment, reproductive toxicity, developmental risk, chronic exposure, children’s vulnerability, or lifelong wireless use.
The FCC’s old limits did not survive court scrutiny
The regulatory story is just as important as the biological story.
In 2021, the U.S. Court of Appeals for the D.C. Circuit remanded the FCC’s decision to keep its 1996 radiofrequency exposure limits unchanged. The court found that the FCC failed to provide a reasoned explanation for its determination that the guidelines adequately protect against harmful effects of radiofrequency exposure unrelated to cancer.
The court specifically faulted the FCC for failing to adequately address evidence involving children, long-term exposure, wireless-device ubiquity, technological developments since 1996, and environmental impacts.
That matters because the public is still living under exposure limits rooted in an earlier technological era. Those limits were developed before today’s saturation of smartphones, Wi-Fi routers, Bluetooth devices, tablets, wearables, smart meters, cell towers, small cells, and 5G infrastructure.
FDA and HHS messaging has shifted
The federal messaging is no longer as stable as the public was led to believe.
In January 2026, Reuters reported that the U.S. Department of Health and Human Services would launch a study on cellphone radiation, and that the FDA had taken down old webpages saying cellphones are not dangerous. HHS said the FDA removed webpages with old conclusions while the department undertook research to identify knowledge gaps involving electromagnetic radiation and modern technologies.
At the same time, the FDA’s current public cell-phone page still contains broad reassurance language, including that “the weight of scientific evidence has not linked cell phone radio frequency radiation with any health problems.”
That contradiction is exactly why the public deserves a full reassessment, not recycled talking points.
The World Health Organization is not the final word
WHO-commissioned reviews are often presented to the public as if they settle the matter. They do not.
The United States formally exited the World Health Organization on January 22, 2026, after HHS cited WHO failures involving COVID-19, lack of reform, and lack of accountability, transparency, and independence.
That political fact is separate from the science, but it matters for public trust. No international body should be treated as above scrutiny, especially when public-health agencies have lagged behind emerging evidence before.
And even within the WHO-commissioned evidence base, the animal-cancer review reported high-certainty evidence for key tumor endpoints in animals.
The real public-health picture
The public has not been given the complete picture.
Here is the complete picture:
Meningioma, the most common brain tumor, has risen sharply in U.S. SEER data. Thyroid cancer has doubled since 2000. Salivary-gland cancer has increased. Glioblastoma shows age-specific increases in young adults and the oldest adults. Pediatric and young-adult central nervous system tumor signals exist. Non-malignant brain tumors, which make up the majority of brain and CNS tumors, have been repeatedly underemphasized in public messaging.
At the same time, the National Toxicology Program found clear evidence of malignant schwannomas and some evidence of gliomas in exposed male rats. A WHO-commissioned animal-cancer review reported high-certainty evidence for heart schwannomas in male rats. Melnick and Moskowitz’s 2026 risk assessment found current exposure limits far above levels estimated to protect against cancer risk and male reproductive harm. The FCC lost in court over its failure to adequately justify keeping old RF limits. FDA/HHS messaging has shifted enough that HHS launched a new review and FDA removed older webpages with outdated conclusions.
That is not an all-clear.
That is a warning signal.
The public does not need panic. The public needs honesty, precaution, and modern regulation. People should not have to wait for decades of additional disease burden before agencies update standards that were never designed around chronic, lifelong, whole-population exposure.
The responsible conclusion is clear: the tumor statistics are real, the animal evidence is serious, the exposure limits are outdated, and blanket reassurances are no longer defensible.






