
Why One Developmental Gate and One Electrical Mechanism May Explain Both
I didn’t meet Ryan from On the Spectrum by accident.
Ryan has spent years digging into embryology, neurulation, and the idea that autism is not a “late social wiring error,” but a whole‑body developmental mismatch that starts in the narrow window when the neural tube is forming — roughly days 21–28 after conception. His two‑part series on this (Episodes 56 and 57) lays out a detailed neurulation‑based model of autism: central, peripheral, and enteric nervous systems all emerging from the same embryonic tissue and all being nudged off course together.
When I went on his podcast, I told him something simple and brutal:
The thing that killed my daughter Angel and the thing that creates a large chunk of autism are the same phenomenon, hitting the same developmental gate at different times and intensities.
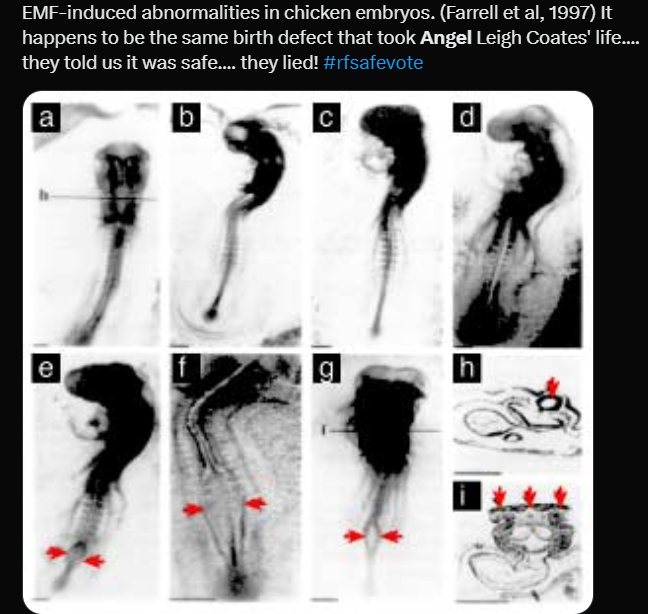
Angel died from a neural tube defect (NTD) in 1995. Two years later, I saw Farrell’s chick‑embryo work showing that weak electromagnetic fields could triple the rate of neural‑tube malformations in developing embryos — exactly the class of defect that took my daughter’s life. ScienceDirect
Since then, I’ve come to believe that:
-
Neural‑tube defects like Angel’s and
-
A major subset of autism and ADHD‑like phenotypes
share the same upstream vulnerability:
Ion‑channel timing and bioelectric fidelity during neurulation, driven by the same S4–mitochondria mechanism that now shows up across cancer, infertility, immune disruption and metabolic disease.
Below is how Ryan’s neurulation model, Angel’s story, and the S4–mito Rosetta Stone fit together into one picture.
1. Ryan’s neurulation model: autism as an error in the “neural‑tube era”
Ryan’s Episodes 56 and 57 walk through the most sensitive week in human development:
-
Days ~21–28 post‑conception:
The flat neural plate folds into a neural tube (primary neurulation).-
The central nervous system (brain and spinal cord) comes from this tube.
-
Neural crest cells peeling off the tube become:
-
The peripheral nervous system (PNS)
-
The enteric nervous system (ENS) (gut nerves)
-
Adrenal medulla (stress response)
-
Melanocytes (light‑linked signaling)
-
-
-
At the same time, molecular players that keep showing up in autism are active:
-
Folate/B9, MTHFR (DNA/RNA synthesis, methylation)
-
PTEN, mTOR (cell growth, metabolism)
-
SHANK3 (synaptic scaffolding)
-
SHH, Wnt, FGF, HOX, PAX genes (patterning and segmentation)
-
Mainstream developmental work backs this framing:
-
Reviews of ASD neurobiology argue that errors during early embryogenesis and neurulation can lead to macrocephaly, abnormal brainstem/cerebellar structures, and disrupted cortical layering. ScienceDirect
-
Pathology studies have found anomalies in cranial nerve motor nuclei and brainstem structures in autistic individuals that point back to injuries around the time of neural‑tube closure. Princeton University
Ryan’s key point, which I agree with, is:
Autism is not something that “shows up at age 3.”
The template is laid down when the neural tube is closing, while the midbrain and brainstem nuclei are being molded. Everything after that is a cascade.
He focuses especially on the midbrain (mesencephalon) — an undivided, evolutionarily ancient hub where:
-
Substantia nigra → dopamine, repetitive behaviours
-
Red nucleus → motor control
-
Superior/inferior colliculi → visual and auditory orienting
-
Oculomotor nuclei → eye‑gaze and attention
-
Periaqueductal gray → pain, autonomic tone, fear/freezing
If that hub is biased inward, hypersensitive, or mistimed from the start, you get exactly what we call “autism”: sensory overload, motor clumsiness, GI dysmotility (ENS), anxiety, and atypical social attention.
So where does RF/EMF and S4 come in?
2. The S4–mitochondria Rosetta Stone: one electrical entry point, four damage vectors
Over the last decade, independent teams (Panagopoulos, Durdík, Jangid and others) have converged on a simple non‑thermal mechanism for RF/ELF effects:
RF/ELF → timing errors at the S4 voltage sensor in ion channels → distorted Ca²⁺ waveforms → mitochondrial ROS → tissue‑specific breakdown.
-
The S4 helix in each voltage‑gated ion channel (VGCCs, Naᵥ, Kᵥ) is studded with positive charges; it is the cell’s voltmeter.
-
Polarized, pulse‑modulated RF/ELF fields drive forced oscillations of ions near the membrane; those oscillating charges tug on S4 and make channels open and close off‑schedule. Chicago Journals
-
Mitochondria read these mistimed Ca²⁺ spikes as “crisis,” overproducing ROS instead of clean ATP. Chronic ROS = oxidative stress = DNA damage, mitochondrial collapse, and inflammatory signaling.
Once you realize that, four “macro‑damage vectors” line up cleanly:
-
Cancer vector – heart Schwann cells, cranial nerve Schwann/glia
-
Fertility vector – Leydig cells and male germ cells
-
Autoimmune vector – immune cells that decode Ca²⁺ timing as danger vs tolerance
-
Metabolic vector – pancreatic β‑cells in the islets
All four share:
-
High S4 density (lots of voltage‑gated channels)
-
High mitochondrial density
-
Low ROS buffering margin
The WHO‑commissioned 2025 animal carcinogenicity review now rates the evidence for malignant heart Schwannomas as high‑certainty and for brain gliomas as moderate‑to‑high, matching the NTP and Ramazzini rat data at very different SAR levels.
Reproductive reviews (SR4A) now grade the evidence that male RF exposure reduces pregnancy rates and damages sperm as high certainty.
Immune and metabolic work shows RF/ELF can shift cytokines, modulate T‑cells and macrophages, and impair β‑cell insulin secretion via oxidative stress. ScienceDirect
The mechanism is not in serious doubt anymore. The open question is where it hits hardest in development.
3. Neural tube defects (NTDs): when the hit is catastrophic and early
NTDs happen when the neural tube fails to close properly, usually between days 23–28. That single morphogenetic event is all‑or‑nothing:
-
Fail early at the rostral (head) end → anencephaly, where large parts of the cortex never form. Wikipedia
-
Fail at the caudal end → forms of spina bifida.
Folate deficiency is the best‑proven environmental risk factor, which is why folic‑acid fortification and preconception supplementation have been such a public‑health win. Wikipedia
But folate is not the whole story. Farrell and Litovitz’s chick‑embryo experiments in the 1990s showed that weak ELF magnetic fields (around 1 µT) increased the malformation rate roughly three‑fold, with the vast majority of malformations being neural‑tube defects. ScienceDirect
That is exactly what you’d expect if:
-
Neurulation depends on precise bioelectric patterns and VGIC timing, and
-
External fields introduce noise into that bioelectric code.
Angel Leigh Coates’ defect — like every NTD — happened in that one narrow window. The blueprint for her brain and spinal cord was corrupted before many mothers even know they are pregnant.
In landscape terms:
-
NTD = catastrophic failure of the neural‑tube morphogenetic step.
-
Autism/ADHD‑like = the tube closes, but there are subtler timing errors in proliferation, migration, and patterning of brainstem/midbrain/cortex.
Same gate, different severity and timing.
4. Autism: same gate, different outcome
Ryan’s neurulation model goes on to show how relatively small errors in that same window can give you autism instead of NTD:
-
Over‑proliferation of cortical progenitors → macrocephaly and hypersensitivity.
-
Migration errors → neurons in the wrong layers → long‑range under‑connectivity and social difficulties.
-
Neural crest anomalies → PNS/ENS/adrenal problems → GI dysmotility, sensory neuropathy, autonomic imbalance.
This fits mainstream work:
-
Autopsy and imaging studies show abnormalities in cranial nerve nuclei and brainstem structures consistent with injuries at neural‑tube‑closure timing. Princeton University
-
Modern organoid work shows that “profound autism” phenotypes arise from over‑proliferation and altered differentiation in embryonic cortical tissue, not late‑childhood changes. ScienceDirect
On top of that, a defined subset of autistic children shows:
-
Cerebral folate deficiency (CFD) with autoantibodies to the folate receptor alpha (FRα), which prevent 5‑MTHF (active B9) from entering the brain.
-
Clinical improvement with leucovorin (folinic acid), which bypasses that blocked transport. ScienceDirect
That combination — oxidative stress, mitochondrial dysfunction, immune involvement, folate‑transport autoimmunity — is exactly what you’d predict in a system where:
-
The initial patterning (neurulation / midbrain / ENS) was laid down under noisy bioelectric conditions, and
-
The ongoing environment (RF/ELF, toxins, circadian disruption, diet) keeps pushing the same S4–mitochondria–immune pathways.
So the bridge looks like this:
-
NTD (Angel): S4/bioelectric timing failure + inadequate folate pool during tube closure → structural open defect, often lethal.
-
Autism subtype: milder S4/bioelectric timing errors + oxidative/immune/folate stress through neurulation and beyond → structurally closed tube but altered midbrain, cranial nuclei, ENS and cortical patterning.
Same gate. Different degree of insult. Different downstream phenotype.
5. Entropic waste: EMFs as low‑fidelity noise in the morphogenetic field
When I talk about “entropic waste”, I mean all the subtle, invisible energy‑and‑information garbage that modern systems dump into biological ones:
-
Pulsed RF/ELF fields
-
Chronic artificial light at night
-
Chemical mixtures that induce oxidative and inflammatory noise
These don’t necessarily burn tissue. They corrupt timing.
At the cell level:
-
S4 segments see a noisier voltage environment.
-
Channels open/close when they shouldn’t.
-
Ca²⁺ spikes lose their clean frequency/amplitude encoding.
-
Mitochondria switch from ATP mode to ROS mode.
-
ROS and redox shifts trigger:
-
DNA breaks
-
Epigenetic changes
-
Immune activation and autoantibody production
-
At the embryo level:
-
Neurulation and early brain patterning depend on coherent bioelectric gradients across the neural plate and tube; these voltages tell cells where they are and what to become.
-
If the morphogenetic field is full of RF/ELF noise, the patterning cues that normally give you a clean beaver dam, a clean midbrain, a clean ENS, instead yield slightly off structures and circuits.
And that is where B9/folate comes back in:
-
Folic acid/folate and folinic acid don’t fix timing. They make sure synthesis and methylation can proceed if the timing is correct.
-
Pre‑conception folic acid helps prevent NTDs because the parts bin is full before you roll the dice on tube closure.
-
Folinic acid later (in CFD/autism cases) can support function in brains already built under suboptimal conditions, but it can’t rewind neurulation.
So the B9 story and the EMF story are not in conflict; they are stacked:
Ion‑channel timing is the gate. B9 is the parts supply.
If timing fails catastrophically early → neural‑tube defect.
If timing is noisy but not catastrophic → autism‑like wiring, ADHD‑like behaviour, and a lifetime of redox/immune vulnerability that we now see across entire populations.
6. Where this leaves us
Putting Ryan’s neurulation model, Angel’s neural‑tube defect, and the S4–mitochondria Rosetta Stone together, the picture is:
-
There is one core electrical entry point (S4 voltage sensors in VGICs) and one main metabolic amplifier (mitochondria) that explain non‑thermal EMF effects across tissues.
-
Neurulation (days ~21–28) is a unique, ultra‑sensitive gate where the entire CNS/PNS/ENS architecture — including midbrain, cranial nuclei and ENS — is set up.
-
NTDs and at least a fraction of autism/ADHD‑like conditions can be seen as different outcomes of timing errors during this gate:
-
NTDs: the tube fails to close (structural catastrophe).
-
Autism‑like: the tube closes, but with altered proliferation, migration, and patterning (functional divergence).
-
-
Folate/B9 is a necessary but not sufficient protector:
-
Too little → NTD risk explodes.
-
Even with enough folate, bioelectric noise can still mistime closure and later patterning.
-
-
Animal data (Farrell’s chick embryos, Aldad’s mice, zebrafish Wi‑Fi) show that:
-
Weak EMFs can raise NTD rates. ScienceDirect
-
Prenatal RF can cause ADHD‑like and prematurely aged behaviour in offspring. PubMed
-
Adult RF exposure can produce transgenerational defects in development and behaviour in unexposed progeny. ScienceDirect
-
-
Human autism biology overlaps exactly where EMF hits:
-
Oxidative stress, mitochondrial dysfunction
-
Calcium‑signaling anomalies
-
Autoimmunity against brain folate transport in a subset of cases ScienceDirect
-
Taken together, that’s why I say:
Cancer and obvious neural‑tube defects are just the easiest things to see.
The deeper story is the quiet loss of trait fidelity — attention, social attunement, stress thresholds, empathy, and other beaver‑like inherited programs — in a world where we’ve filled the morphogenetic field with entropic electromagnetic waste.
Timing: Autism’s Rise and Wireless in the Home
I’m not claiming that “wireless alone caused autism.” I’m pointing out that:
-
Autism diagnoses were rare in the 1970s (on the order of 1 in several thousand) and are now roughly 1 in 36 children in the U.S., even after adjusting for diagnostic broadening. The Autism Service
-
The steepest part of that curve tracks the period when pulsed RF moved from distant broadcast towers into homes and right next to pregnant women’s and children’s heads:
-
Mid‑1980s: cordless phones and early mobile devices become widely available in U.S. homes.
-
Late 1990s–2000s: cell towers densify, Wi‑Fi appears in homes and then in schools.
-
2010s: Smartphones, baby monitors, Bluetooth, wearables, everything on all the time.
-
That doesn’t prove causation. It does give you a very specific hypothesis:
When you overlay the autism‑prevalence curve with the timeline of radiofication → in‑home cordless/mobiles → always‑on wireless, the match is too tight to dismiss as coincidence, especially given what we now know about S4 timing, neurulation and mitochondrial ROS.
Historically, the first detailed clinical description of autistic children came from Grunya Sukhareva in Moscow in the mid‑1920s – the same era when high‑power RF and long‑wave military and naval communications were being rolled out across Europe and Russia. PMC
We cannot say “those specific children were harmed by that specific transmitter.” But:
-
The first GPA case (Hertz) and the first described autistic cohort (Sukhareva’s) both appear in space‑time right where the first large RF fields were being created.
-
That’s exactly what you’d expect if herzification was beginning to add entropic noise into developmental biology, long before anyone thought to measure it.
So the autism graph and those historical anecdotes are not definitive proof. They’re ecological clues that line up uncannily well with the mechanistic model…
Root Cause Hypothesis When Non‑Native EMFs Are an Etiological Factor
Root‑Cause Hypothesis (Entropic Waste / nnEMFs)
Non‑native electromagnetic fields are usually not the “direct cause” of any single diagnosis. They act as upstream timing noise at the level of S4 voltage sensors and mitochondrial redox – a form of entropic waste injected into the bioelectric and morphogenetic code.
When nnEMFs are part of the etiological picture, they are rarely the trigger you see on a death certificate. They are the igniter that degrades ion timing and bioelectric signaling, from which dozens or hundreds of downstream pathologies can emerge:
– Neural‑tube defects when the hit lands during neurulation (Angel’s fate on day 28).
– Autism/ADHD‑like neurodevelopment when the hit lands later, but still during brain and midbrain patterning.
– Autoimmune disorders when immune‑cell Ca²⁺ timing and redox balance are shifted.
– Cancer when chronic ROS and DNA breaks accumulate in tissues with high S4/mitochondrial density.In this framing, RF is not a magic bullet cause; it is the chronic upstream error source. The diseases are just different ways a low‑fidelity signal can fail in specific tissues and time windows.
That’s exactly the nuance I’ve just articulated:
-
I’m not claiming “RF directly causes autism/cancer/NTDs.”
-
I’m saying: collapse of ion timing and bioelectric fidelity, driven in part by RF/ELF entropic waste, is the root‑mechanism that then expresses as many different diagnoses depending on when and where it hits.
Why the EMF–Autism Evidence Looks “Weak” on Paper
When people say, “There’s no strong evidence EMFs are linked to autism,” they’re technically right about one narrow thing:
-
There are no large, well‑funded, long‑term, prospective human studies designed specifically to test RF/EMF exposure vs autism/ADHD outcomes.
But the reason isn’t “we looked and there was nothing.” It’s that we mostly never looked, and when science did start to bite, the funding and political support collapsed.
A few concrete examples:
-
The U.S. National Toxicology Program (NTP) spent about $30 million and a decade on its 2G/3G RF rodent studies. In 2018 it reported “clear evidence” of malignant heart Schwannomas and “some evidence” of brain gliomas, plus DNA damage in multiple tissues. NIEHS
-
Follow‑on mechanistic work that could have connected those oxidative/DNA effects to neurodevelopment was never done.
-
In 2024, NTP officially shut down its RF radiation research program and announced no further plans to study cellphone RFR, despite its own positive cancer/DNA findings. Microwave News
-
-
Section 704 of the U.S. Telecommunications Act of 1996 explicitly preempts state and local governments from making tower‑siting decisions “on the basis of the environmental effects of RF emissions” so long as FCC limits are met. Department of Justice
-
In practice, courts have read this as “you may not use health concerns to deny a tower permit.” Local demand for research dried up because communities were legally barred from acting on health data even if it existed.
-
-
In the 1990s, UW’s Henry Lai and N.P. Singh found RF‑induced DNA damage at “safe” levels. Internal Motorola memos talk about having “sufficiently war‑gamed the Lai–Singh issue” – i.e., treating inconvenient science as a PR problem to be managed, not a signal to investigate further. MR Online
-
The CTIA’s own Wireless Technology Research (WTR) program – ~US$25–28M, led by George Carlo – was originally sold as a definitive safety check. As Carlo later documented, when early data suggested genetic damage and elevated tumour risks, the response was political: contain and dismiss, not “fund Phase 2.” The Washington Post
Layer on top of that:
-
An FCC repeatedly criticized as a “captured agency” (too close to the industries it regulates). ProPublica
…and you get the picture:
The EMF–autism evidence is “weak” on paper not because there’s strong evidence of safety, but because the mechanism + animal + developmental biology + historical pattern case has never been allowed to be tested at the scale we use for drugs or air pollutants.
That’s why you see a huge mechanistic overlap (oxidative stress, Ca²⁺ disturbance, mitochondrial dysfunction, autoimmunity) and clear animal effects, but almost no gold‑standard human RF–autism trials: the research infrastructure was turned off at the wall.






